Torque Release Technique (TRT)
Spinal Torque and Structural Correction
 The bones of the spine house the spinal cord. The spinal cord has a loose covering called the “Meninges“. The outer layer, the “Dura Mater” is a tough and non-stretchy robust membrane that attaches to the spine in only a few key places. It also forms a sleeve about the nerves as they exit from the spine.
The bones of the spine house the spinal cord. The spinal cord has a loose covering called the “Meninges“. The outer layer, the “Dura Mater” is a tough and non-stretchy robust membrane that attaches to the spine in only a few key places. It also forms a sleeve about the nerves as they exit from the spine.
These attachment points become very important in that if there is a subluxation (misalignment that causes nerve interference/miscommunication) at these locations, the tugging effect on the nerves and the torque or twisting of the Dura (Meninges) causes somewhere between 7 to 12 other subluxations to occur (8 on average)(1). This situation not only distorts the spine but induces stresses in the other important systems of the body and often causes structural imbalance in the form of nerve tension which in turn brings about abnormal muscle tensions. These are called “Primary Subluxations”.
The end result is some part of your health is “switched off”.
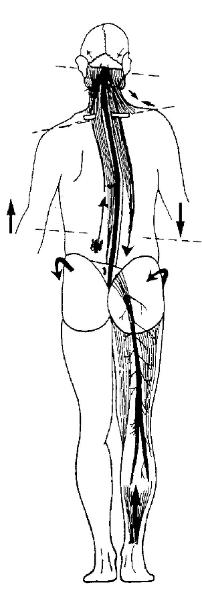
Using this system of Chiropractic spinal correction called Torque Release Technique, these tensions of the spine and spinal cord and changes in muscle tension are most easily monitored at the feet. Here predictable patterns of change in tension can be discerned.
The analysis of the tension in the Meninges is performed by testing the tension in the feet and legs. You will notice that I spend quite a bit of time touching and pressing on the feet. When I do that what I am also doing is not only assessing the tension in the feet but also the tension transmitted from the meninges as well as the spinal cord.
(See diagram at left for an idea of how the spinal tension relates to foot tension.)
By applying small pressures to the key points of the spine especially where the Meninges attach to the spine, it is possible to determine the precise place where adjustments will have the greatest beneficial change.
When the precise location and direction of forces necessary to make a correction are determined, it is possible to use relatively small force corrections to achieve the desired changes in the spine to alter large patterns of structural distortions (7 to 12 changes for each correction with an average of 8). These corrections are done using mechanical devices, one called the “Integrator” and the other the “Activator”. Corrections can also be made using gentle sustained finger pressure using a breathing pattern assist.
“Primary” Subluxations
The places in the spine where the meninges attach to the spine are the locations where major structural distortion can arise from. I view these as major release points for correction.
The symptoms a person experiences are often a result of the presence of the “Primary
subluxations” (meningeal attachment locations) and the “secondary subluxations” that they cause to form as a result of the presence of a Primary subluxation.
When the Primary subluxation is corrected, the secondary subluxations will most often also be resolved. If the primary subluxation is not corrected and only the secondaries are corrected then eventually the long list of secondaries will eventually return.
Once one primary subluxation is corrected, like pealing off a layer of onion, another less severe, but still important hither to hidden Primary Subluxation surfaces. This also needs to be adjusted into a better functioning state.
“Less” can be “more”
In reality, for each primary subluxation adjusted there are on average 8 other changes that are also taking place. With 3 primaries being adjusted, it means that we expect 27 changes on average to happen. (3 Primaries + their 24 Secondaries). NOT all of the spinal bones need to move but some spinal bones move more than once
This is a lot of change to set in motion. When a person first starts to have the Torque Release adjustments, if the person is not as fit as they really need to be, then some “response changes” may be experienced after the first or second adjustment session.
Responses
Most people’s response to adjustments is a sense that your body is working better than it used to.
Not everyone experiences a symptomatic response to subluxations being adjusted. For those who do, they may feel achy and sore as if they have done a lot of sport without going into training first.
When this happens it is NOT that something has gone wrong with the adjustment. Rather it indicates that the adjustment has worked very well. It is just that parts of your body which have not worked properly for some time, are now working with greater vigour. Your body is merely not used to this sudden change and renewed activity and it needs to be fitter.
Those who do will feel this sort of response will do so often one to three days after the first or second adjustment. Commonly it will last for 2 to 3 days, gradually fading away.
Celebrate
Rather than worry about this change, see it for what it really is. Your body is working better.
It can be uncomfortable, but it is a natural, understandable and beneficial physiological process. Celebrate the fact that better function has returned to your body!
Resolve to keep your body improving by keeping to your adjustment schedule and following the advice given to you. This way you and I can work to keep that improvement moving towards the peak improvement that is possible for you.
Your body can then start to repair, become more stable, become more comfortable and life can become more productive and also more enjoyable.
What is this thing with the feet?
As adjustments proceed, you will notice that I often do things to your feet. You might ask yourself “….What on earth is he doing with my feet?”
The answer to that question is that I am judging the tension within muscles that relates to the changes in the signaling they receive from nerves that are irritated as a result of a subluxation pattern. This pattern of tension was first noted by Dr van Rumpt. Dr Holder, the developer of TRT, went on to perfect this tension measuring method.
See diagram at left for an idea of how the spinal tension relates to foot tension.
This altered tension is a hint to the presence of “primary” subluxations. These are re-checked for each subluxation. Each time a subluxation is corrected, the analysis goes back to step one. That is, is there a sign of increased tension on one side of the body, does it change with head rotation. If the answer to these questions is yes, then the pattern that presents is tested to see what would relieve that pattern.
From this “non-linear” approach, we always adjust the segment which presents the body with the greatest amount of distortion first. This may or may not relate to the symptoms you came in to
have attended to. But it will always have the greatest impact on your ability to self correct. And isn’t
that why you have come in for care? The fact that your body has not been able to “fix itself”.
So while your conscious educated mind may want pain or discomfort to go away, your body may be demanding that some other much more important process be set right first.
That is why “patients” need to be “patient” and work with me to help you – “the whole person you”, make a recovery. After all if you were only after pain relief, you would have taken a pill a pill for the pain. That would be much cheaper, but probably not as good for you, only cheaper. Well we both know that is not why you are reading this page and why you may have want to come to me as a chiropractor for.
How Torque Release Technique started
You may be interested to know that Dr Jay Holder DC, MD always wanted to be a chiropractor.
Unfortunately he did not have the funds to put himself through the training. He said that he researched funding that was available, and found that the military and police forces would fund further education after a certain amount of service. He joined the police force in Miami. He was in the drug squad doing work similar to that depicted on the TV show “Miami Vice”. Dr Holder then went on to graduate as a chiropractor and then on to earn his medical degree.
As a medical doctor, he runs 2 drug rehabilitation clinics. The treatment modalities employed in the drug rehabilitation setting are chiropractic, auriculotheraphy, nutrition and counseling. Dr Holder is on record as stating that if he could do only one thing for a patient seeing him for rehabilitation, then that would be chiropractic adjustments of the spine. (1)
Drug Rehab effectiveness in the USA is judged by retention rates of the “inmates” in the program.
Dr Holders retention rates far exceeded the norms. The treatment intervention was so “novel” in the usual sense of what is expected, that Dr Holder was asked to do a study that would verify that chiropractic care was a valid treatment “for drug rehabilitation”.
Holder in an attempt to validate chiropractic care in the field of drug rehabilitation undertook a study that eventually showed that chiropractic is indeed a useful treatment in this setting.
For the study, Holder developed a technique that is completely reproducible. He went to the extent of developing the integrator. This is an instrument which in the hands of chiropractors, repeatably simulates the actions of a chiropractor’s hands as they adjust the spinal subluxations. The Torque Release Technique is the only chiropractic technique that was developed for a clinical trial. It also makes it possible for practitioners to reproduce their findings before an adjustment is given as well as give exactly the same adjustment under the same set of circumstances.
Torque Release Technique is based on the important contributions of Doctors: Palmer (Upper Cervical Specific), Van Rumpt (DNFT), Toftness, DeJarnette(SOT), Thompson, Epstein (Network) and Logan and is a synthesis of the reasoning behind the techniques they developed. The work of these chiropractors has stood out as making an outstanding and long lasting contribution to not only the profession but also to alleviating the suffering of humanity.
References
(1) Torque Release Technique seminars Melbourne 2003, Sydney 2004.
Links
Other reading about research related to Torque Release Technique and articles that have flowed from the original research.